![]()
PRACTICE CHANGES / UPDATES
Tina Waugh, MD of Lahey Health Primary Care, Beverly has opened her patient panel.
Susan DeLuca, MD of Lahey Health Primary Care, Beverly resigned effective June 6, 2021.
Effective 8/1/2021, Michael Edwards, MD will be relocating from Patton Park Medical, 42 Asbury Street, South Hamilton to Emtar Health Care, 205 Willow St Suite C-1-C, South Hamilton Phone: 978-468-1918 Fax: 978-468-8095.
PROVIDER DIRECTORY
Did you know you can use our website to search for a NEPHO Provider? Go to NEPHO.com/provider-directory. You can search by name, specialty, or location.
NEW PROVIDERS
Rosa Bui, MD
North Shore GI
100 Cummings Center Suite 107 C
Beverly, MA 01915
Phone: 978-232-1120
Fax: 978-232-0110
Rebecca Calder, PDM
Beverly Podiatry
900 Cummings Center Suite 309 V
Beverly, MA 01915
Phone: 978-922-0288
Fax: 978-927-6265
Maria “Mary” Lonshteyn, MD
North Shore GI
100 Cummings Center Suite 107 C
Beverly, MA 01915
Phone: 978-232-1120
Fax: 978-232-0110
Marguerite Sullivan, MD
Massachusetts Dermatology Associates
900 Cummings Center Suite 311T
Beverly, MA 01915
Phone: 978-225-3376
Fax: 978-560-1245
SAVE THE DATE
Coding and Billing Webinar
Date: Wednesday, July 14, 2021 @11:30am–12:30pm
Coding and Billing – Sneak Peek at 2022
Location: GoogleMeet Conference Call
RSVP: Margaret.M.Doyon@Lahey.org
Coding and Billing Webinar
Date: Wednesday, August 11, 2021 @11:30am–12:30pm
ICD-11 Overview
Location: GoogleMeet Conference Call
RSVP: Margaret.M.Doyon@Lahey.org
NP/PA MEETING
Date: Wednesday, September 8th @ Noon
Location: GoogleMeet Conference Call
RSVP: Stephanie.K.Cunningam@Lahey.org
or 978-236-1753
Coding and Billing Webinar
Date: Wednesday, September 8, 2021 @11:30am–12:30pm
Title: TBD
Location: GoogleMeet Conference Call
RSVP: Margaret.M.Doyon@Lahey.org
New Physician Orientation
Date: Thursday, July 29 @ 7:30 am
Location: GoogleMeet Conference Call
RSVP: Alycia.Messelaar@Lahey.org or 978-236-1784
Office Manager Meeting
Date: Wednesday, September 15, 2021 @ Noon
Location: GoogleMeet Conference Call
RSVP: Alycia.Messelaar@Lahey.org or 978-236-1784
NECOMG 2021 ANNUAL MEETING SUMMARY
The NECoMG 2021 Annual Meeting was held on Thursday, June17th at 7:00a.m. The meeting was held virtually via GoogleMeet. The meeting details include the following:
- There were over 120 attendees
- The following physicians have been voted to another 3 year term as Board of Directors:
- Dr. Kathryn Hollett
- Dr. Richard Mugge
- Dr. Eric Sleeper
Our guest speaker was Dr. Leslie Sebba, retired Chief Medical Officer of Beth Israel Lahey Health Performance and former Medical Director for the NEPHO.
Dr. Sebba presented on the Current State of Clinically Integrated Networks in Massachusetts. He discussed the increasing healthcare costs for Massachusetts families and the pressure for providers to lower healthcare costs and improve quality performance.
He discussed Physician Group margins for 2020 as well as Hospital margins after COVID relief fund distribution. Dr. Sebba highlighted the importance of working as a system for infrastructure support, technical assistance and coordination with providers.
He stated that BILHPN is well positioned to perform well in risk based contracts and shared an overview of the new structure and resources dedicated to contracting and performance improvement.
The Annual Meeting attendance was tracked using an online evaluation form that was sent to all physicians after the meeting. The evaluation form included a section to allow for questions and sharing updates about practice changes. NEPHO will analyze all responses and follow up on the questions.
PHILIPS ISSUES RECALL NOTIFICATION
Philips issues recall notification* to mitigate potential health risks related to the sound abatement foam component in certain sleep and respiratory care devices.
To read the Press Release, click here.
* This is a recall notification for the US only, and a field safety notice for the rest of the world
NEW PPE GUIDANCE
DPH issued this guidance document that discusses the universal use of facemasks, eye protection, isolation gowns, and more. The state expects facilities to implement the changes no later than July 1.
Among the changes, eye protection is no longer needed for every patient encounter but is limited to circumstances where healthcare personnel are caring for confirmed or suspected COVID-19 cases. DPH also clarifies facemask use for source control and transmission-based precautions.
PODS AND IPA MEETING KEY TAKEAWAYS
Quality
- Data on NEPHO performance on the BILH System Diabetes Composite was shared, along with the ongoing interventions targeted to improve performance.
- The diabetes composite includes annual eye exam, A1c < 9, and BP<140/<90.
- The goal is to have all 3 in control by August 31.
- EPIC users: There is an updated smartphrase to document home BPs: .BPREMOTEDOCU
- Office colleagues other than clinicians can call the patient and record the information (the clinician does not need to be the documenter).
Patient Experience
- A 3 part webinar patient experience refresher series is being offered for providers during June and July.
- The webinars are approved for risk management training.
- The webinars will be recorded and available for distribution.
- Refresher course for office colleagues is being explored as a next webinar series.
Provider Experience
- A summary of April Practice meetings was shared.
- Discussion was invited on which provider experience improvement tasks are achievable, and the scope and timeline for actionable tasks.
Pharmacy
- A case based discussion on inhalers was shared along with tools to identify coverage and assist with inhaler selection.
Informational
- Detail on types of discharges that qualify for Transitional Care Management (TCM) Visits/coding was shared.
- This is part of an ongoing effort to share FAQs and answers from pods and IPA meetings.
PAYOR UPDATES
Blue Cross Blue Shield of Massachusetts
Portal Now Open for Cancer Care Authorizations
To prepare provider’s practice for the Quality Care Cancer Program, BCBSMA wants providers to be aware of the latest tools, resources, and trainings available. As a reminder, the program requires providers to request authorization for certain outpatient medical oncology and radiation oncology services. The program is administered by AIM Specialty Health. To view the complete notification, click here.
Authorization Requests Streamlined for Some Outpatient Surgeries
As of June 30, 2021, Authorization Manager will allow requesters to complete the InterQual medical necessity checklist for certain procedures (back surgery, hip surgery, knee surgery, hysterectomy) performed in an outpatient setting. To view the complete notification, click here.
Change to Telehealth Cost Share and Authorization Requirements
Effective July 1, 2021, BCBSMA will reinstate member copayments, co-insurance, and deductibles for non-COVID telehealth visits, including all mental and behavioral health services.
Resuming Authorization Processes
In alignment with guidance from the Division of Insurance, we have resumed the normal authorization processes for all services for our commercial and Federal Employee Program members, and will start requiring authorization for Medicare Advantage members on July 1, 2021.
We will continue to waive the authorization requirement for commercial and Medicare Advantage initial requests for the following services with a COVID diagnosis:
- Emergent inpatient services
- Skilled nursing, rehab, and long-term acute care
- Home health care
To view the complete notification, click here.
Harvard Pilgrim Health Care
Payment Policy Update: Nutrition Counseling
Harvard Pilgrim Health Care has updated the Nutritional Counseling Payment Policy. For additional information and to view the notification, click here.
Outpatient Oncology Authorization Program
As a reminder, for our commercial and Medicare Advantage members, prior authorization is required from Harvard Pilgrim’s vendor partner Oncology Analytics for outpatient chemotherapy (infused and/or injected) and radiation therapy. Oncology Analytics conducts medical review of chemotherapeutic protocols (chemotherapy, support and symptom management drugs) and radiation treatment plans for Harvard Pilgrim members with a cancer diagnosis that requires these services. To view the updates, click here.
Payment Policy Review and Integration
As part of the integration work as a combined organization, Harvard Pilgrim is reviewing and assessing existing Harvard Pilgrim Health Care and Tufts Health Plan Payment Policies, both as part of the typical annual review and to assess opportunities for consistency. The Plan expects this work to continue over the course of the next year. The policies listed below are scheduled for review over the next few months. Harvard Pilgrim will keep providers and office staff well informed of any changes and will continue to provide timely notice for any payment policy updates via Network Matters. For additional information and to view the notification, click here.
MassHealth
The state’s Executive Office of Health & Human Services (EOHHS) has issued this list of program flexibilities that MassHealth promulgated during the COVID-19 state of emergency. Now that the emergency declaration has been lifted in the state, and as the federal public health emergency continues, some of the flexibilities have also been lifted while others have been extended.
“This document is not meant to be an exhaustive list of programmatic changes but is instead focused on changes that pertain to managed care plans,” EOHHS wrote.
Medicare
MACs Resume Medical Review on a Post-payment Basis
Beginning August 2020, Medicare Administrative Contractors (MACs) resumed post-payment reviews of items and services with dates of service before March 2020. MACs may now begin conducting post-payment medical reviews for later dates of service. The Targeted Probe and Educate program (intensive education to assess provider compliance through up to 3 rounds of review) will restart later. The MACs will continue to offer detailed review decisions and education as appropriate. To view the notification, click here and locate the article by title.
Quarterly Update to the Medicare Physician Fee Schedule Database
This article informs providers of the July 2021 updates of the 2021 MPFS. Make sure the billing staffs are aware of these updates. To view the MLN Matters article, click here.
Tufts Health Plan
Evaluation and Management Professional Payment Policy Update
Tufts updated the payment policy for annual wellness visit claim edits for Senior Products. To view the complete policy, click here.
Tufts Medicare Preferred
As a result of the 5-Star rating* given to the Tufts Medicare Preferred HMO plans by Medicare, your eligible patients can enroll in these plans all year long. Tufts Health Plan achieved a 5-Star CMS Quality rating for 2021 — now for six years in a row! Tufts Health Plan is one of only two plans in the country to achieve 5 Stars for six consecutive years. What does this mean for your patients and our members?
Our 5-Star rating gives patients the freedom of a special election period where they can enroll into one of our plans outside of Medicare’s Annual Election Period. Tufts Medicare Preferred HMO and Senior Care Options plans received 5 stars in several measures including:
- Staying Healthy: Screenings, Tests and Vaccines
- Member Experience with Health Plan
- Health Plan Customer Service
What this means for members is they are not obligated to remain in whatever plan chosen. If life changes and a member needs new/different coverage, our 5-star rating gives the freedom to use one additional opportunity (outside of the annual enrollment period) to move to one of our other plans.
We have the largest Medicare Advantage membership in Massachusetts, with 97% of our members staying with us year after year. In these uncertain times, Tufts Health Plan Medicare Preferred HMO is a 5-Star rated plan you can trust.
A few more updates and reminders:
July & August virtual meeting registration information can be found here www.thpmp.org/meetings and dates & times are as follows. CMS permits you to distribute this information to patients via email and in office material including flyers which are attached.
- Monday, July 12, 2021 – 10:00am (Virtual Medicare Meeting – Enrollment)
- Thursday, July 15, 2021 – 10:00am (Virtual Medicare 101 – Educational)
- Thursday, July 15, 2021 – 4:00pm ( Virtual Medicare Meeting – Enrollment)
- Monday, July 19, 2021 – 10:00am (Virtual Medicare Meeting – Enrollment)
- Tuesday, July 20, 2021 – 4:00pm (Virtual Medicare 101 – Educational)
- Wednesday, July 21, 2021 – 10:00am (Virtual Medicare Meeting – Enrollment)
- Monday, July 26, 2021 – 10:00am (Virtual Medicare Meeting – Enrollment)
- Tuesday, July 27, 2021 – 10:00am (Virtual Medicare Meeting – Enrollment)
- Wednesday, July 28, 2021 – 10:00am (Virtual Medicare Meeting – Enrollment)
- Tuesday, August 10, 2021 – 10:00am (Virtual Medicare Meeting – Enrollment)
- Thursday, August 12, 2021 – 10:00am (Virtual Medicare 101 – Educational)
- Tuesday, August 17, 2021 – 10:00am (Virtual Medicare Meeting – Enrollment)
- Wednesday, August 18, 2021 – 10:00am (Virtual Medicare Meeting – Enrollment)
- Wednesday, August 18, 2021 – 4:00pm (Virtual Medicare 101 – Educational)
- Thursday, August 19, 2021 – 10:00am (Virtual Medicare Meeting – Enrollment)
- Monday, August 23, 2021 – 4:00pm (Virtual Medicare Meeting – Enrollment)
- Tuesday, August 24, 2021 – 10:00am (Virtual Medicare Meeting – Enrollment)
- Wednesday, August 25, 2021 – 10:00am (Virtual Medicare 101 – Educational)
- Thursday, August 26, 2021 – 10:00am (Virtual Medicare 101 – Educational)
For the most up-to-date information about Tufts Health Plan’s policies and coverage pertaining to COVID-19 including testing and treatment, telehealth, billing guidelines, etc., please refer to: https://tuftshealthplan.com/covid-19/provider/coronavirus-updates-for-providers
We also offer Tufts Medicare Preferred Supplement plans and, for participating providers, Tufts Health Plan Senior Care Options (SCO). Tufts Health Plan SCO (which also has a 5-Star rating) may be a great option for patients who are 65+ and on MassHealth Standard and continues to offer monthly enrollment. With SCO, members get more benefits than MassHealth and Original Medicare, plus free extras, all at no cost. If you have questions or need digital or physical marketing materials for your practices, please contact Marcel Philippe, Manager of Business Development at Marcel_Philippe@tufts-health.com or 617-417-2587.
Harvard Pilgrim Health Care / Tufts Health Plan
Point32Health brings together two of New England’s top health plans
Harvard Pilgrim Health Care and Tufts Health Plan today announced the name of its parent organization, Point32Health. Inspired by the 32 points on a compass, our new name represents the role the organization plays in guiding and empowering our 2.2 million members and making a meaningful impact across the health care industry.
As Point32Health, we will continue to deliver the trusted, high-quality services our members expect and demand, with a reinvigorated focus on creating a new health care journey that is more personal and seamless than ever before. As a leading health and well-being organization with 90 years of combined service, Point32Health makes it our purpose to guide and empower healthier lives for everyone — regardless of age, health, race, identity or income — by working differently.
While Point32Health is the name of our parent organization, the Harvard Pilgrim Health Care and Tufts Health Plan brands will continue to appear in the marketplace for the foreseeable future.
The announcement of our new organization’s name and brand marks the beginning of our future and further solidifies who we are and the value we deliver in the marketplace.
PROVIDER RELATIONS
Things are constantly changing within NEPHO practices – it truly is inevitable. As a reminder, please reach out to the Provider Relations Department periodically to request updates or assistance in creating provider lists. Examples of frequent outreach we receive include and are not limited to:
- Primary Care Providers with open panels for patients transitioning out of Pediatric care
- Primary Care Providers with open panels for Special Needs patients transitioning out of Pediatric care
- NEPHO PCP practice rosters used to update EMR mapping tied to billing/ referral network identification
Please do not hesitate to reach out to Alycia.Messelaar@lahey.org for such requests. We are here to help bring ease to both the practices and the patients you serve.

Please CLICK HERE to take a moment to read the Provider Spotlight on Dr. Jeffrey Rubel of Beth Israel Lahey Health Primary Care and Specialty Care Beverly Medical Associates.
Please CLICK HERE to take a moment to read the Provider Spotlight on Dr. Rebecca Calder of Beverly Podiatry Associates.
If you would like to be featured on the PHO website, please reach out to Alycia Messelaar Alycia.Messelaar@Lahey.org or 978-236-1784.

Please click here to view our newest Virtual Networking video from Dr. Howard Goldberg of Howard Goldberg, MD, Inc.
Additional Virtual Networking videos from NEPHO providers can be found here.
Please reach out to Alycia.Messelaar@lahey.org if you are interested in being featured in a Provider Spotlight or Virtual Networking video.
REFERRAL MANAGEMENT
Tufts Health Plan reinstates referral requirements July 1, 2021
Tufts Health Plan has stated that referral requirements will be reinstated for all products as outlined below:
- Tufts Health Commercial Plan: Effective for dates of service on or after July 1, 2021
- Senior (Tufts Medicare Preferred and SCO) Products: Upon the end of the Federal public health emergency
- Tufts Together: Effective for dates of service on or after August 7, 2021
- Note: Tufts Health Together* and Tufts Health Direct* do not require in network referrals.
* please refer to health plan directory for in network specialist participation
As a reminder BILHPN Referral Simplification for Tufts HMO/POS, BCBS HMO/POS, HPHC HMO/POS remains in place and eliminates the need for an administrative referral from PCPs in the BILHPN network for specialty office visits within the Northeast PHO/BILHPN network.
- Any referrals to a Specialist outside the Northeast PHO (NEPHO) network will need to be reviewed by the Medical Director.
Please continue to fax or submit your out of PHO referrals through your EMR system to the NEPHO for review.
Out of PHO referrals require 5-7 days for review.
Please review the list of contracted health plans included within the referral simplification program.
- US Family Health* and Tufts Freedom Plan* are excluded from Referral simplification and will require referrals to in- network specialists
* please refer to health plan directory for in network specialist participation
The PHO Referral Management team is here to help with specialty referrals. As a reminder, referral requests outside of the Northeast PHO should be reviewed by our team. We have many new specialists in the Northeast PHO and we are learning more about the new specialists coming into the BILH network. We can help you find the appropriate provider to care for your patients.
Please send all out of PHO referral requests to our dedicated fax line at 978-236-1611. If you have any questions or need an urgent referral to a specialist, please contact Ann Cabral, Referral Manager at Ann.Cabral@Lahey.org or 978-236-1758.
PHARMACY
There are two BILHPN Pharmacy Newsletters this month.
Please click here to be directed to the BILHPN June 2021 Newsletter “Inhaler Resources”.
Please click here to be directed to the BILHPN June 2021 Newsletter “Inhalers: More Info, UPDATED: T2DM Medication Coverage Chart and MassHealth RX Copay Changes”.
For more information or questions, please contact Carol Freedman, NEPHO Pharmacy Manager at carol.freedman@lahey.org or 978-380-4089.
QUALITY
The BILH system ambulatory quality goal is a composite measure to improve the care of patients with diabetes. The three measures in the composite are diabetic eye exams, blood pressure at goal (less than 140/less than 90), and A1c less than 9.
Why is this goal worth paying attention to?
The evidence behind the goal is compelling: Studies have shown that risk factor control is highly effective in reducing cardiovascular events in patients with Type 2 diabetes (BARI 2D, JACC 2015). Studies have also shown the excessive cardiovascular risk that is associated with the number of risk factors outside of target ranges (NEJM, 2018; 379:633-634).
Our local data shows we have room for improvement: Preliminary data for 2021 shows that only 9% of BCBS HMO patients tracking to NEPHO providers currently have all 3 risk factors in the diabetes composite met or in control.
The BILH system timeline is to get patients in control/to goal before August 31st. Below are a few tips to help your patients meet their goals. Please reach out to the NEPHO Quality team if you have additional suggestions or would like more information.
- Primary Care Providers
- Use your PHO EMR alerts – PHO analysts have identified which risk factor(s) your patients need to get into control.
- If the EMR alert says they are due for an eye exam, please encourage your patient to schedule the exam.
- If it is clinically appropriate, consider medication adjustments for patients who have not met their blood pressure or A1c targets, and schedule them before they leave your office for an early follow up visit.
- Some patients may value your written instructions. Consider “prescribing” diabetes eye exam AND extracting a commitment from your patient for when they will schedule the exam (“I would like you to call today to schedule the appointment, are you able to do that?”)
- PCP Office Managers and Key Quality Contacts
- Check your “Needs Appointments” lists: PHO analysts are leveraging Arcadia reporting weekly to identify diabetes patients who need appointments and sending these names to office managers and key contacts. Try to book these patients for office visits prior to August 31st if possible.
- Alert your MAs and nurses that patients who have BPs readings above 140/above 90 should get a second reading, preferably towards the end of the visit.
- For Ophthalmology/Endocrinology/Cardiology/Nephrology practices
- Please obtain and document second BP for your patients who have above 140/above 90 initial readings.
- Please reach out to patients who miss their appointments to re-schedule.
POPULATION HEALTH
Reminder Diabetic Eye Exams
The BILH Ambulatory DM Composite Measure includes diabetic eye exams. Please see the Quality Section of this newsletter for an explanation of the DM Composite Measure.
The NEPHO Quality Team has taken the following steps to help improve our DM Eye Exam compliance rate:
- Names of patients with an existing network provider relationship were sent to their eye care providers. These providers will reach out to their patients and try to schedule exams.
- Our Commercial Case Manager, Jean St. Peter, is assisting with outreach to patients who are due for eye exams.
- BILHPN will be sending letters to patients for practices who are using EPIC. The NEPHO Quality Team will send letters for the non-Epic practices.
- Eye Exams are highlighted as part of the DCCP Pre-Visit Planning Pilot.
According to the National Eye Institute (NEI) Diabetic retinopathy is a leading cause of blindness in American adults and is the most common diabetic disease. An estimated 40 to 45% of diabetic Americans experience some stage of diabetic retinopathy. From 2010 to 2050, the number of Americans with diabetic retinopathy is expected to nearly double, from 7.7 million to 14.6 million. Hispanic Americans are expected to see the greatest increase in cases, rising more than three-fold from 1.2 million to 5.3 million.
- No Warning Signs – 50% of patients are not getting their eyes examined or are diagnosed too late for treatment to be effective. Patients normally don’t experience symptoms until their vision is already damaged.
- Vision loss and blindness – Diabetic retinopathy usually affects both eyes by damaging the retina. Over time, the blood vessels protecting the retina become blocked causing vision blurriness or loss. If left untreated, it could ultimately lead to blindness.
- Annual comprehensive eye exams are crucial – A dilated eye exam allows for an eye care professional to notice the early warning signs for this disease and prevent vision loss. Timely treatment and appropriate follow-up care can reduce the risk of blindness by 95%
- Refer your patients to an eye care provider today – You can find a detailed list of in-network providers via https://www.nepho.org/provider-directory/.
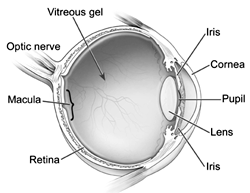
Diabetic eye disease can affect many parts of the eye, including the retina, macula, lens and the optic nerve.
Please contact Laureen Viel, Lead Population Health Specialist at 978-236-1746 or laureen.viel@lahey.org with questions or concerns.
CODING TIP OF THE MONTH
OPTUM Newsletter – June 2021 | Dementia and Alzheimer’s Disease
Medical Necessity Helps Support Evaluation and Management (E/M) Leveling
It has been 6 months since the new Evaluation and Management (E/M) updates became effective. Providers no longer have to include history and exam components in documentation to determine the E/M code level for the office/outpatient CPT codes 99202-99215. Instead they are now using updated guidance for determining the level of service based on either time or Medical Decision Making (MDM).
Though E/M guidelines have changed, medical necessity has not. The importance of supporting medical necessity by documentation is still an element of E/M coding guidelines. Although the history and physical exam are no longer required to level the visit, they are still important components in establishing medical necessity, supporting medical decision making, and providing quality care. Documenting these components helps maintain continuity of care and assists other providers in management of patient care.
Medical necessity determines coverage and level of reimbursement from Medicare and the other payers:
Medicare
- requires that the level of service provided must be supported by medical necessity.
- defines medical necessity as health-care services or supplies needed to diagnose or treat an illness or injury, condition, disease, or its symptoms and that meet accepted standards of medicine.
- determines, on a case-by-case basis, if the method of treating a patient is reasonable and necessary.
Payers
- provide coverage for care, items and services that they consider to be medically necessary.
- limit coverage, even if a service is reasonable and necessary, if the service is provided more frequently than allowed under a national coverage policy, a local medical policy, or a clinically accepted standard of practice.
- use National Correct Coding Initiative (NCCI) claim edits to ensure that payment is made for specific procedure codes when provided for a patient with a specific diagnosis code or predetermined range of ICD-10-CM codes. ICD-10-CM codes should support medical necessity for any services reported.
As we move forward with the implementation of the new E/M updates for outpatient services it is important to remember how medical necessity must be supported by documentation. This includes services based on time and on the MDM. To better support medical necessity for services reported, the following principles should be followed:
- List the principal diagnosis, condition, problem, or other reason for the medical service or procedure
- Example: Chief Complaint/Reason for Visits
- Assign the diagnosis code to the highest level of specificity
- Example: Diabetes with Complications should be coded to the highest specificity
- For office and/or outpatient services, never use a “rule-out” statement (a suspected but not confirmed diagnosis); a clerical error could permanently tag a patient with a condition that does not exist
- Example: Patient seen in ED for racing heart– this is a new condition but ED provider added anxiety diagnosis to chart and prescribed Zoloft. Patient followed up with PCP and it was found the patient had a mini stroke. The anxiety is a suspect condition captured in the ED. Anxiety should not be captured on the problem list as a chronic treated condition. Anxiety is a suspect condition.
- Distinguish between acute and chronic conditions, when appropriate
- Example: Acute conditions are severe and sudden in onset. This could describe anything from a broken bone to an asthma attack. A chronic condition, by contrast is a long-developing syndrome, such as osteoporosis or asthma.
- Identify how injuries occur
- Example: Patient fell off bike and fractured hip
As we move forward into 2021 keeping medical necessity as a driving component when leveling E/M services ensures new guidelines are being followed and captured compliantly.
Please reach out to Shawn Bromley at 978-236-1704 or shawn.m.bromley@lahey.org if you have additional questions related to medical necessity and importance it has in supporting E/M leveling for outpatient services.
PATIENT EXPERIENCE COMMENTS
Blackburn Primary Care, Gloucester – 1 Blackburn Drive
- Dr. Jay Isaac and Beth are the best doctors ever. They care about their patients.
Danvers Family Doctors PC, Danvers 140 Commonwealth Avenue
I Love Dr. Subroto Bhattacharya. Great and respectful staff. He gives me peace
Lahey Primary Care, Beverly – 30 Tozer Road
- Dr. Tina Waugh is an incredible diagnostician and is able to know me very well. She is always prompt and super caring.
Lahey Primary Care, Beverly – 100 Cummings Center
- Dr. Khalil Shahin listened to my concerns and responded with options that made me feel I could take part in my health care.
Lahey Primary Care, Beverly – 900 Cummings Center
- Dr. Daniel McCullough is a true gentleman and is certainly on top of his game concerning health issues.
Lahey Primary Care, Danvers – 5 Federal Street
- Dr. Mauri Cohen is a doctor that is very easy to talk to about any medical conditions. There are doctors that want to talk more than listen, but Dr. Cohen definitely listens which makes me feel comfortable.
- Very good experience with Dr. Brent Fryling.
Lahey Primary Care, Manchester – 192 School Street
- Dr. Matthew Plosker is very competent and personable. I trust him implicitly and have recommended him.
PRACTICE RECOGNITION
The Northeast PHO recognizes colleagues who provide a positive experience for our patients, help us keep care local and meet our quality targets.
This month’s winner is:
Regina Moormann, Danvers Family Doctors.
Regina Moormann, Danvers Family Doctors, was recognized for efforts to support NEPHO and other practices learn about practice management systems.

Regina Moormann, Danvers Family Doctors
Please let us know if you would like to nominate a team member in your practice or another practice for the recognition program. We will deliver gift cards to the winners each month, and they will be announced here and in our website “Hot Topics” section.